Transient Myeloproliferative Disorder Associated with Trisomy 21
Slovakia
Type your case report here.



Type your content here.
Background
Transient myeloproliferative disorder (TMD), also known as transient abnormal myelopoiesis (TAM), is a clonal, self-limited proliferation of immature megakaryoblasts that occurs almost exclusively in fetuses and neonates with trisomy 21 (Down syndrome) [1, 4]. It represents a unique preleukemic state that shares morphologic and molecular features with acute megakaryoblastic leukemia (AMKL), but unlike AMKL, it typically regresses spontaneously within the first three months of life [4]. The condition is detected in approximately 4–10% of neonates with Down syndrome and may also occur in cases of mosaic or partial trisomy 21 [4, 6]. The underlying mechanism involves a constitutional trisomy 21 combined with a somatic mutation of the GATA1 gene, resulting in the production of a truncated transcription factor (GATA1s) that promotes proliferation of megakaryocytic precursors and suppresses normal erythroid differentiation [4]. In the fetal and perinatal period, the disease can manifest as fetal hepatosplenomegaly, hydrops fetalis, polyhydramnios, or placentomegaly [2, 3]. The enlarged fetal liver, often hyperechogenic, reflects massive extramedullary hematopoiesis and infiltration by megakaryoblasts. Splenic enlargement and occasional ascites or pericardial effusion may accompany the picture. Doppler studies may show increased middle cerebral artery peak systolic velocity due to fetal anemia [3, 5]. Cytologically, peripheral blood and fetal liver aspirates reveal increased circulating blasts, often with megakaryoblastic morphology (irregular nuclei, cytoplasmic blebs, and platelet peroxidase positivity). Bone marrow may be normocellular or show hypocellularity with increased immature megakaryocytes [4]. While spontaneous remission is typical, about 20–30% of infants who survive the neonatal period later develop acute megakaryoblastic leukemia (AMKL), typically within the first four years of life [4]. Thus, even though the prenatal or neonatal presentation may be self-limited, long-term hematologic follow-up is essential. From the prenatal diagnostic viewpoint, the combination of trisomy 21 and hepatosplenomegaly on ultrasound should prompt suspicion of TMD [1, 2]. Differentiation from other causes of fetal organomegaly such as intrauterine infections, lysosomal storage disorders, or immune hydrops is crucial [3, 5]. Amniocentesis or cordocentesis can confirm the chromosomal abnormality and hematologic features, allowing accurate counseling and prognostication.
Case Summary
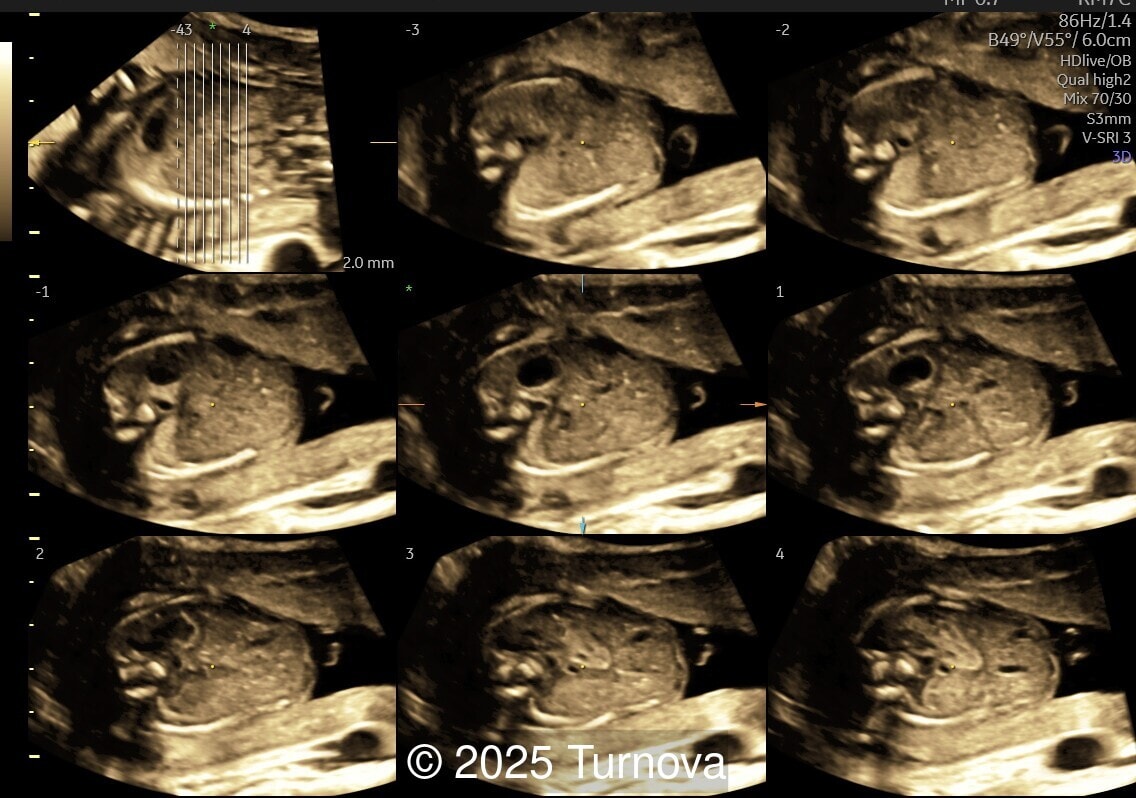
A 32-year-old gravida 2, para 1 presented at 19 + 0 weeks of gestation for a routine second-trimester screening ultrasound. Ultrasound examination revealed abnormal subcutaneous tissue and abnormal nuchal fold highly suggestive of trisomy 21. In addition, a marked hepatomegaly was noted, with the liver appearing diffusely hyperechogenic. No ascites or signs of hydrops were present.
Given the constellation of findings, trisomy 21 with associated hematologic involvement – most likely transient myeloproliferative disorder – was suspected. The patient underwent amniocentesis, which confirmed full trisomy 21. After multidisciplinary counseling, the patient opted for termination of pregnancy for medical indication, which was performed at 20 + 2 weeks of gestation. A fetal autopsy was performed. External examination confirmed facial dysmorphism characteristic of Down syndrome, including a flat nasal bridge and epicanthic folds. Internal examination revealed marked hepatosplenomegaly. The liver was enlarged (weighing approximately 2.5 times the expected weight for gestational age) and demonstrated diffuse pale nodularity. Histopathologic examination showed massive extramedullary hematopoiesis with numerous immature megakaryoblasts, large atypical nuclei, and frequent mitotic figures within the hepatic sinusoids and portal areas. Similar infiltrates were present in the splenic red pulp and occasionally in the bone marrow, confirming the diagnosis of transient myeloproliferative disorder in association with trisomy 21. This case underscores the importance of recognizing fetal hepatomegaly with dysmorphic features of trisomy 21 as a potential marker of TMD, prompting targeted cytogenetic testing and appropriate counseling.
References
1. Hartung J, Chaoui R, Wauer R, Bollmann R. Fetal hepatosplenomegaly: an isolated sonographic sign of trisomy 21 in a case of myeloproliferative disorder. Ultrasound Obstet Gynecol. 1998; 11(6): 453-5.
2. Macones GA, Johnson A, Tilley D, Wade R, Wapner R. Fetal hepatosplenomegaly associated with transient myeloproliferative disorder in trisomy 21. Fetal Diagn Ther. 1995; 10(2): 131-3.
3. Smrček JM, Baschat AA, Germer U, Gloeckner-Hofmann K, Gembruch U. Fetal hydrops and hepatosplenomegaly in the second half of pregnancy: a sign of myeloproliferative disorder in fetuses with trisomy 21. Ultrasound Obstet Gynecol. 2001; 17(5): 403-9.
4. O’Connell AE. Perinatal Transient Myeloproliferative Disorder in Trisomy 21. NeoReviews. 2016; 17(11): e636-e644.
5. Kim YH et al. Prenatal Manifestation of Transient Abnormal Myelopoiesis: hepatosplenomegaly as a key marker. Korean J Radiol. 2009; 10(2): 190-194.
Walasik I et al. Prenatal Manifestation of Transient Abnormal Myelopoiesis: hepatos
View the Answer Hide the Answer
Answer
Type your case answer report here. ...
Background
Transient myeloproliferative disorder (TMD), also known as transient abnormal myelopoiesis (TAM), is a clonal, self-limited proliferation of immature megakaryoblasts that occurs almost exclusively in fetuses and neonates with trisomy 21 (Down syndrome) [1, 4]. It represents a unique preleukemic state that shares morphologic and molecular features with acute megakaryoblastic leukemia (AMKL), but unlike AMKL, it typically regresses spontaneously within the first three months of life [4]. The condition is detected in approximately 4–10% of neonates with Down syndrome and may also occur in cases of mosaic or partial trisomy 21 [4, 6]. The underlying mechanism involves a constitutional trisomy 21 combined with a somatic mutation of the GATA1 gene, resulting in the production of a truncated transcription factor (GATA1s) that promotes proliferation of megakaryocytic precursors and suppresses normal erythroid differentiation [4]. In the fetal and perinatal period, the disease can manifest as fetal hepatosplenomegaly, hydrops fetalis, polyhydramnios, or placentomegaly [2, 3]. The enlarged fetal liver, often hyperechogenic, reflects massive extramedullary hematopoiesis and infiltration by megakaryoblasts. Splenic enlargement and occasional ascites or pericardial effusion may accompany the picture. Doppler studies may show increased middle cerebral artery peak systolic velocity due to fetal anemia [3, 5]. Cytologically, peripheral blood and fetal liver aspirates reveal increased circulating blasts, often with megakaryoblastic morphology (irregular nuclei, cytoplasmic blebs, and platelet peroxidase positivity). Bone marrow may be normocellular or show hypocellularity with increased immature megakaryocytes [4]. While spontaneous remission is typical, about 20–30% of infants who survive the neonatal period later develop acute megakaryoblastic leukemia (AMKL), typically within the first four years of life [4]. Thus, even though the prenatal or neonatal presentation may be self-limited, long-term hematologic follow-up is essential. From the prenatal diagnostic viewpoint, the combination of trisomy 21 and hepatosplenomegaly on ultrasound should prompt suspicion of TMD [1, 2]. Differentiation from other causes of fetal organomegaly such as intrauterine infections, lysosomal storage disorders, or immune hydrops is crucial [3, 5]. Amniocentesis or cordocentesis can confirm the chromosomal abnormality and hematologic features, allowing accurate counseling and prognostication.
References
1. Hartung J, Chaoui R, Wauer R, Bollmann R. Fetal hepatosplenomegaly: an isolated sonographic sign of trisomy 21 in a case of myeloproliferative disorder. Ultrasound Obstet Gynecol. 1998; 11(6): 453-5.
2. Macones GA, Johnson A, Tilley D, Wade R, Wapner R. Fetal hepatosplenomegaly associated with transient myeloproliferative disorder in trisomy 21. Fetal Diagn Ther. 1995; 10(2): 131-3.
3. Smrček JM, Baschat AA, Germer U, Gloeckner-Hofmann K, Gembruch U. Fetal hydrops and hepatosplenomegaly in the second half of pregnancy: a sign of myeloproliferative disorder in fetuses with trisomy 21. Ultrasound Obstet Gynecol. 2001; 17(5): 403-9.
4. O’Connell AE. Perinatal Transient Myeloproliferative Disorder in Trisomy 21. NeoReviews. 2016; 17(11): e636-e644.
5. Kim YH et al. Prenatal Manifestation of Transient Abnormal Myelopoiesis: hepatosplenomegaly as a key marker. Korean J Radiol. 2009; 10(2): 190-194.
Walasik I et al. Prenatal Manifestation of Transient Abnormal Myelopoiesis: hepatos
Discussion Board
We appreciate your patience as we review all submitted answers. Check back soon to see if you were correct!