Case of the Week #597
(1) UT Southwestern Medical Center, Dallas, Texas, United States of America; (2) Femicare, Center of prenatal ultrasonographic diagnostics, Martin, Slovakia.
A 23-year-old, G1P0, woman presented to our maternal fetal medicine unit at 22 weeks, 3 days for a follow-up fetal anatomic survey. The fetus was female with low-risk noninvasive prenatal testing. The following findings were observed.



The following images were obtained at 35 weeks, 6 days gestation.




View the Answer Hide the Answer
Answer
We present a case of single left superior vena cava. This was an isolated finding. No other cardiac, or extracardiac anomalies were found. Our diagnosis was confirmed after birth.
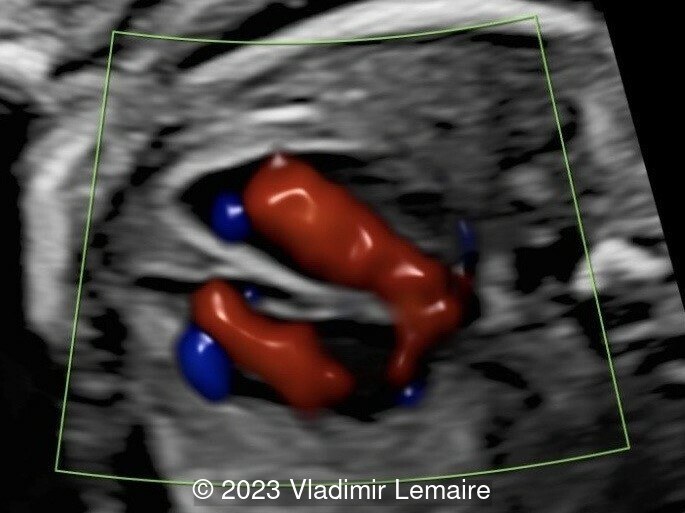
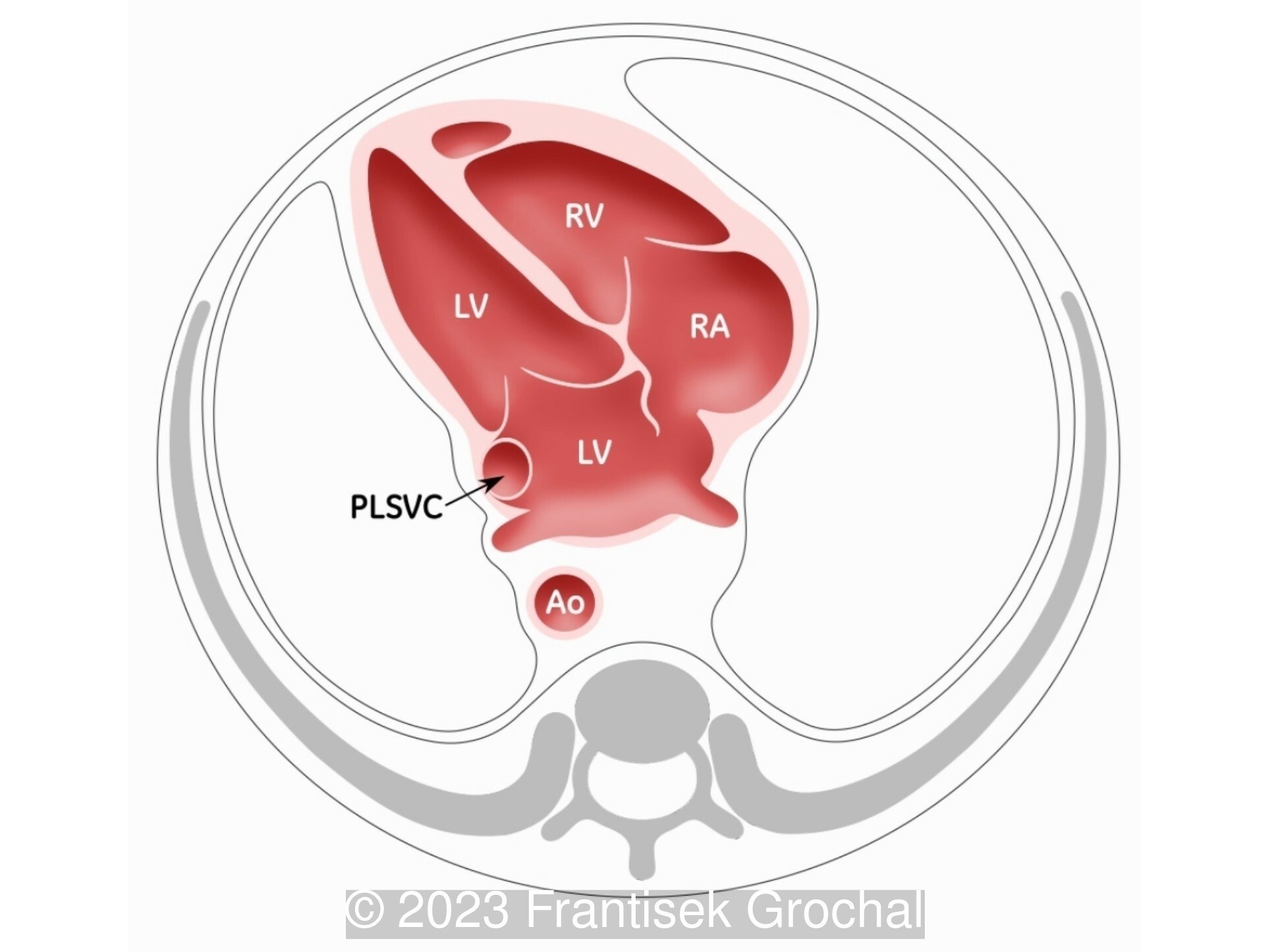
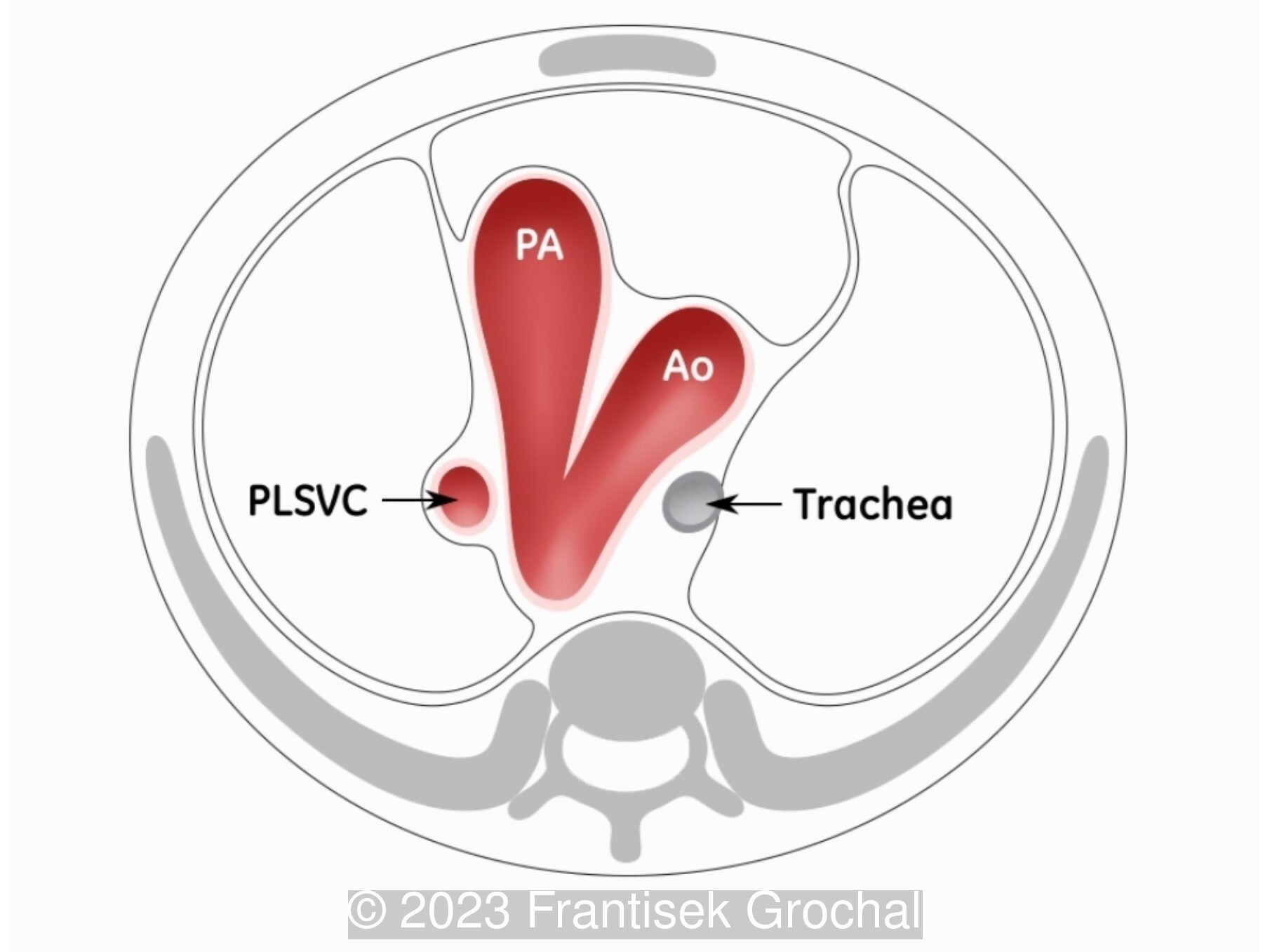
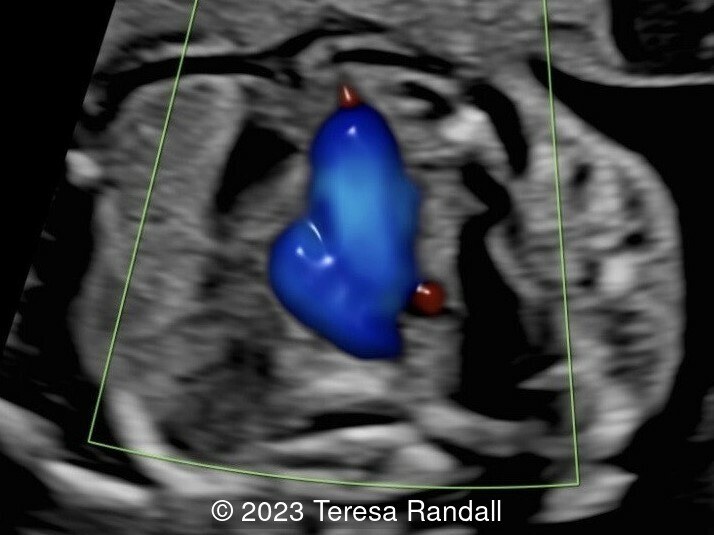
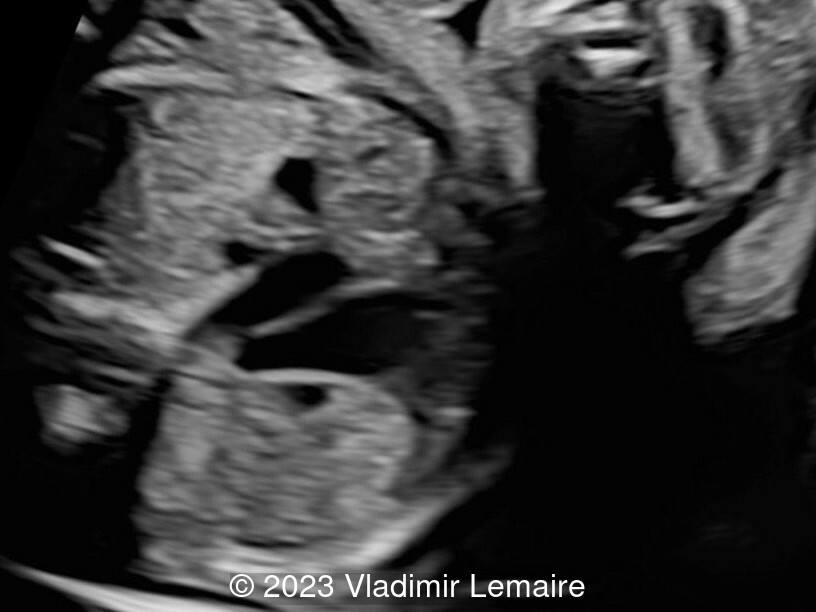
The ultrasound evaluation demonstrated that the situs was solitus. At the level of the four-chamber view, the left superior vena cava can be seen in cross-section at the border of the left atrium. Two pulmonary veins can also be seen draining into the left atrium which rules out a total anomalous pulmonary venous connection, supracardiac type 1. At the level of the right ventricular outflow tract (RVOT), three-vessel view (3VV), and three-vessel-trachea view (3VTV), instead of seeing four vessels with the additional vessel to the left of the pulmonary trunk, only three vessels are seen in an abnormal configuration. From left to right, the persistent left superior vena cava, ductal arch, and aortic arch were demonstrated. The innominate vein was also documented coursing from right to left, instead of its normal left-to-right trajectory. The coronary sinus was dilated during the growth scan at 35 weeks, 6 days.
- Image 5: Right ventricular outflow tract at 35 weeks of gestation.
- Image 6: Three-vessel view at 35 weeks of gestation.
- Image 7: Three-vessel-trachea view at 35 weeks of gestation. It is important not to confuse the trachea with the right superior vena cava.
- Image 8: Dilated coronary sinus at 35 weeks of gestation.



Discussion
During embryogenesis, systemic venous drainage involves two pairs of cardinal veins. The anterior cardinal veins drain the cranial parts of the embryo, and the posterior cardinal veins drain its caudal parts. By eight weeks of gestation, the right anterior cardinal vein forms the right superior vena cava, and the left brachiocephalic vein, while the left anterior cardinal vein regresses to become the ligament of Marshall. Failure of regression of the left cardinal vein results in the formation of the left superior vena cava which usually courses between the left atrial appendage and the left pulmonary veins and enters an enlarged coronary sinus. On rare occasions, the right anterior cardinal vein regresses. This results in an absent right superior vena cava and a persistent left superior vena cava. A condition also referred to as a single left superior vena cava.
As reported by Guzzetti et al, a persistent left superior vena cava with an absent right superior vena cava is an extremely rare combination, occurring in 0.05 to 0.1 % of cases with situs solitus.
Differential diagnosis includes bilateral superior vena cava and total anomalous pulmonary venous connection, supracardiac type 1. It is important not to confuse the trachea with the right superior vena cava. With bilateral superior vena cava, the left brachiocephalic vein is usually not seen. Whereas in total anomalous pulmonary venous connection, supracardiac type 1, the left brachiocephalic vein is dilated.
The absence of the right superior vena cava is a common feature of heterotaxy syndrome. When isolated, however, this condition is usually asymptomatic with no hemodynamic effects.

References
[1] Abuhamad A, et al. "The Left Brachiocephalic Vein." A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts (4th edition). Singapore: Wolters Kluwer, 2022. pgs 131-132.
[2] Clur S, et al. Absent right and persistent left superior vena cava, a cause for fetal ventricular disproportion. Ultrasound Obstet Gynecol. 2007; 30: 547-653.
[3] Guzzetti L, et al. Prenatal diagnosis of persistent left and absent right superior vena cava at 21 weeks of gestation. Ultrasound Obstet Gynecol. 2007; 30: 547-653.
[4] Lopes K, et al. Single left superior vena cava: antenatal diagnosis, associated anomalies and outcomes. Ultrasound Obstet Gynecol. 2022; 60: 640-645.[5] Saha S, et al. Persistent left superior vena cava - considerations in fetal, pediatric and adult populations. Australas J Ultrasound Med. 2012; 15 (2): 61-66.
Discussion Board
We appreciate your patience as we review all submitted answers. Check back soon to see if you were correct!